Health-Care Patient-Room HVAC Airflow Patterns


Although satisfying overall air-change rates in health-care patient rooms ensures heating, cooling, and ventilation requirements are met, the flow path of supply air within these spaces determines air-temperature distribution, thermal comfort, air quality, and the potential for the transmission of airborne pathogens. Airflow patterns in a patient room depend on a number of factors, including location and type of supply diffusers, supply-airflow (air-change) rates and associated diffuser throws, supply-air temperature, room-return size and location, bathroom-exhaust-flow rate, location and strength of heat sources, arrangement of furniture and other obstructions to airflow, and location of the patient.
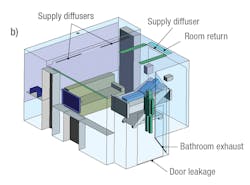
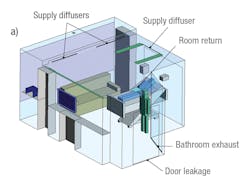
To understand how HVAC configuration can affect airflow patterns, temperature distribution, and the transmission of airborne pathogens, a virtual patient room was created with the help of computational fluid dynamics (CFD). The three-dimensional CFD model included a seating area, a door to the corridor, a door to the bathroom, and supply- and return-air locations. Analysis was performed for two HVAC configurations; in one, the air return was placed near the room door, and in the other, it was placed over the patient’s head (Figure 1). The room contained several pieces of heat-generating equipment, including lighting, a monitor, an infusion pump, a television, and a computer. The room contained two occupants: a patient and a caregiver.
Valuable Insights (Case 1)
Air in the virtual patient room was supplied through three single-slot linear diffusers. Two of the linear diffusers were located near the window to direct supply air toward the window’s glazing to address solar heat gain, while the other was placed over the patient to supply air to the room. The room was assumed to operate under slightly negative pressure, with exhaust flow from the bathroom exhaust fan.
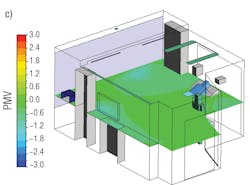
Thermal comfort was analyzed using the Predicted Mean Vote (PMV) index per ANSI/ASHRAE Standard 55, Thermal Environmental Conditions for Human Occupancy. The flow of airborne pathogens was predicted based on trajectories of airflow from the patient’s face.
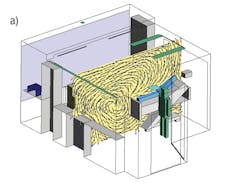
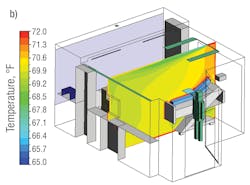
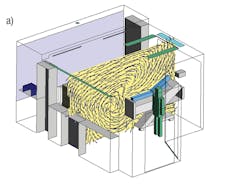
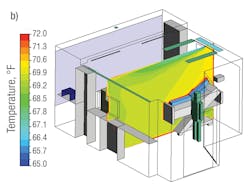
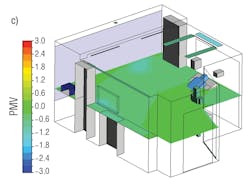
In the case in which the return grill was located near the door, the air exiting the supply diffuser formed a strong recirculating pattern over the patient and behind the bed. As a result, air flowed upward over the patient and was pulled back into the supply-air stream. This recirculation created a slightly higher air-temperature zone near the patient’s head. PMV varied from −3 (too cold) to +3 (too hot). A PMV of 0 indicates a thermally comfortable environment, which is indicated by the color green in Figure 2c. At a height of 4 ft from the floor, occupant thermal comfort was neutral (PMV close to 0.0). However, airborne pathogens released from the patient’s face could get pulled into the supply-air stream and spread throughout the room.
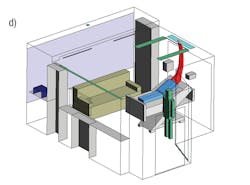
Ideally, supply air from the diffusers should have passed over the patient and returned through the return grill in a single pass without entering the supply stream and recirculating into the room. In an attempt to achieve this, the return grill was increased in size and placed behind the linear diffuser over the patient’s head to provide a path for airborne pathogens to easily exit the room.
Valuable Insights (Case 2)
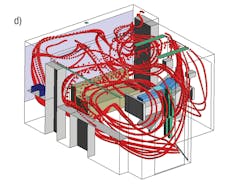
As shown in Figure 3, such modifications achieved temperature distribution and thermal comfort similar to that in the previous case, but significantly changed the flow path of airborne pathogens. In this case, supply air still moved over the patient, but did not get pulled back into the supply-air stream. The return air carrying airborne pathogens found the path of least resistance, readily exiting the room without recirculating. Additionally, hot air behind the patient also exited the room. In both cases, the air-change rate was the same.
Summary
A virtual patient room was created with the help of CFD to evaluate the impact of return-grill location. The analyses provided valuable insight into airflow patterns, temperature distribution, thermal comfort, and, perhaps most importantly, the probable path of airborne particles (pathogens). The traditional practice of placing the return grill near the room door can pull airborne pathogens released from a patient’s face back into the supply-air stream and spread them throughout the room. Simply moving/locating the room return grill directly behind the linear supply diffuser over the patient’s head can lead to a cleaner environment by providing a pathway for airborne pathogens to easily exit the room, which can avoid recirculation of contaminated air back into the room. Importantly, this can be achieved without increasing air-change rates. This analysis demonstrates that air-change rate alone may not be enough in determining the performance of HVAC designs. The flow path of air can play an important role, and it should be analyzed during the early stages of the design process.
It should be noted a combination of factors, including the location and type of supply diffusers, the location of the room return, the supply-air flow rate, and the location of the bathroom exhaust through the door undercut, can affect airflow patterns, which are quite complex and specific to a particular design configuration. Thus, it is difficult to reach general conclusions about the optimization of HVAC configurations for patient rooms. This study, however, demonstrates CFD analysis can be a valuable tool for gaining insight into and optimizing HVAC configurations for improved thermal comfort and the best possible hygiene in health-care facilities.
A specialist in computational fluid dynamics, Kishor Khankari, PhD, is president of AnSight LLC, provider of engineering insights through physics-based simulation and analysis. Over the years, he has provided consulting services that have resulted in the development of solutions to a wide variety of engineering problems related to fluid flow, heat transfer, mass transfer, and similar processes. He is an ASHRAE Distinguished Lecturer; the chair of ASHRAE Technical Committee 9.11, Clean Spaces; a member of ASHRAE’s Research Administration Committee; and a member of the board of governors and a past president of ASHRAE’s Detroit chapter. He can be reached at [email protected].
Did you find this article useful? Send comments and suggestions to Executive Editor Scott Arnold at [email protected].
About the Author
KISHOR KHANKARI, PhD, AnSight LLC, Ann Arbor, Mich.
Dr. Kishor Khankari is president and founder of AnSight LLC. As a specialist in Computational Fluid Dynamics (CFD). he has several years of experience in providing consulting services that have resulted in optimized solutions to a wide variety of engineering problems. Kishor has a Ph.D. in CFD from the University of Minnesota and has regularly published in several technical journals. An ASHRAE Fellow and ASHRAE Distinguished Lecturer, he is a recipient of the ASHRAE Distinguished and Exceptional Service Award; past President of ASHRAE Detroit Chapter, past Chair of ASHRAE Research Administration Committee (RAC) and many other esteemed positions and service to the industry.
HPAC contributions
Aerodynamic Containment Can Reduce Indoor Spread of Infectious Aerosols | HPAC Engineering
Health-Care Patient-Room HVAC Airflow Patterns | HPAC Engineering